Bebo is completely obsessed with her body size, making her a fitness freak who will do anything to maintain her envious figure. When Kareena Kapoor was young, she was quite plump and this must be possibly the reason why she strives so hard to maintain that hot body of hers.
Category: articles
Religious OCD: ‘I’m going to hell’
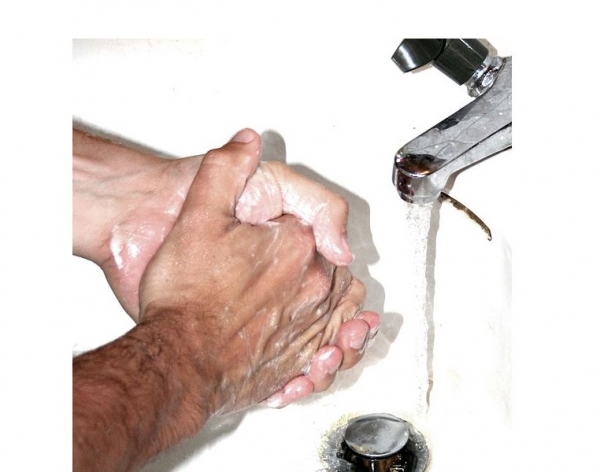
When she was 12, Jennifer Traig’s hands were red and raw from washing them so much. She’d start scrubbing a half an hour before dinner; when she was done, she’d hold her hands up like a surgeon until her family sat down to eat.
Her handwashing compulsions began at the time she was studying for her Bat Mitzvah. She was so worried about being exposed to pork fumes that she cleaned her shoes and barrettes in a washing machine.
“Like a lot of people with OCD, I tended to obsess about cleanliness,” said Traig, now 42. “But because I was reading various Torah portions, I was obsessed with a biblical definition of cleanliness.”
Family dinners were awkward for Tina Fariss Barbour, too, as an adolescent. She would concentrate so hard on praying for forgiveness that if anyone tried to interrupt her thoughts, she wouldn’t respond.
“First I had to get rid of all my sins, ask forgiveness, do it in the right way, and then I had to pray for protection,” said Barbour, now 50. “Or, if something bad happened to my family, it would be my fault because I had not prayed good enough.”
The women come from different faith backgrounds: Barbour is Methodist and Traig is Jewish. But as children they believed fervently that they needed to conduct their own rituals and prayers, or else disaster would befall their families.
Both women say they suffered from a form of obsessive-compulsive disorder known as scrupulosity. A fear of sin or punishment from deities characterizes this condition, said Jonathan Abramowitz, professor and associate chairman of the department of psychology at the University of North Carolina, Chapel Hill.
Obsessive Compulsive Disorder, or OCD, involves unwanted thoughts (“obsessions”) and accompanying behaviors called compulsions that patients use to reduce anxiety. In scrupulosity, the obsessions have a religious or moral underpinning.
Patients with scrupulosity often describe how they believe their thoughts are morally equivalent to actions, Abramowitz said. Psychologists call this phenomenon “thought-action fusion.”
“Scrupulosity literally means ‘fearing sin where there is none,’ ” Abramowitz and colleague Ryan Jacoby wrote in a recent article.
How common is this condition?
Scrupulosity is an understudied subcategory of OCD. Attempts at characterizing how many people might have this disorder, from the 1990s and early 2000s, suggested that somewhere between 5% and 33% of OCD patients have religious obsessions. Scientists are not sure what causes OCD, but they believe a combination of genetic and environmental factors may be at play.
In societies where religiosity is more stringent, the numbers are higher: 50% of OCD patients in Saudi Arabia and 60% in Egypt said they had religious obsessions, according to studies from the early 1990s.
A small number of people with scrupulosity are not religious at all, and a fear of moral transgression or inadvertently offending others weighs on their conscience, Abramowitz said.
Psychologists do not believe that religion causes people to develop OCD. However, religion may influence whether someone with OCD experiences obsessions and compulsions related to religion, Abramowitz said.
A tendency to get anxious and difficulties with uncertainty may factor into the condition, Abramowitz said. And, he pointed out, the vast majority of religious people do not have OCD.
Many “scrupulous” people Abramowitz has met consider religion to be an important part of their lives, but they may avoid institutions such as churches, synagogues or mosques because it reminds them too much of their anxieties.
“They’re walking around with this black cloud of ‘I’m going to hell,’ ” Abramowitz said.
Such a cloud has been been present for centuries. The OCD History Website cites passages from the first century priest and essayist Plutarch and sixth century monk John Climacus that could be interpreted as descriptions of scrupulosity.
St. Ignatius of Loyola, founder of the Jesuits, who died in 1556, appears to have suffered from the condition, said William Van Ornum, professor of psychology at Marist College. Ignatius wrote about his fears about stepping on something that looked like a cross.
There have also been suggestions that Martin Luther experienced scrupulous obsessions, Van Ornum said.
Robert Waters, a retired Lutheran minister, runs an online support network called The Scrupe Group. He said it has about 1,000 members, including Christians of several denominations, Jews, and at least one Hindu and one Muslim. Waters, who has suffered from scrupulosity personally, offers pastoral advice, but also tries to help people overcome their distrust of their own judgment.
“I think that’s really a major part of it: To get to the point where people form their own consciences and don’t rely on other people’s,” he said.
Did I do it right?
Scrupulosity often involves a lot of checking, Abramowitz said. Patients experience distress around the idea that they may have done something wrong or improper, so they may consult the Bible or religious authority figures often to see if they’re doing things right. Consulting people and books isn’t pathological, but in scrupulosity the behavior of checking is excessive compared to other religious people.
Anxious parents often have anxious children, study shows
By Emily Hales
Posted May. 29, 2014 @ 12:01 am
Updated May 29, 2014 at 10:56 AM
Saratoga: Therapy center focuses on anxiety, OCD issues
A new treatment center in Saratoga helps local adults, children and teens dealing with anxiety and obsessive-compulsive disorder receive counseling and therapy services.
Laura Johnson opened the Cognitive Behavior Therapy Center of Silicon Valley in March to treat anxiety and obsessive-compulsive disorders using a scientifically based approach.
The facility is the only place in the South Bay focusing exclusively on anxiety and OCD and offering evidence-based treatments, according to Johnson.
“It’s a very practical, goal-oriented type of therapy that focuses on things people want to change,” Johnson said. “We do a lot of progress monitoring to make sure the therapy is appropriately tailored to the client.”
Therapists work with patients that have OCD and OCD spectrum disorders such as trichotillomania (hair pulling), chronic skin picking, hypochondriasis or health anxiety, eating disorders, body dysmorphic disorder and tic disorders or Tourette syndrome.
“We work with helping build awareness around these habits and behaviors and help them learn new compatible ways to respond,” said Johnson. “We kind of retrain them.”
Teenagers often come in for social anxiety, but the disorder affects people of all ages, said Johnson. To help those patients, therapists will work on helping patients get over their fear of judgment.
Selective mutism is among the more common conditions that afflict younger children, especially girls, Johnson said. A child with selective mutism may be completely silent at school but outgoing and speaks freely at home.
“That’s a really hard one to work with,” Johnson said, adding that in this scenario, therapists will work with parents on gradually exposing their children to different scenarios to get them comfortable with speaking in public.
Panic disorders, post-traumatic stress disorder, agoraphobia and other phobias, anxiety-related insomnia and depression are other conditions that therapists focus on. Each is handled in a different way, and treatment can stretch beyond sessions with a therapist. In that way, therapists tend to be more like teachers and coaches, Johnson said.
“We really train our clients on techniques they can implement at home, outside the session,” Johnson said. “There’s always homework to do.”
Johnson, who resides in Los Gatos, founded the center four years ago in San Jose, but realized she had to move to a bigger location when her business grew and she no longer could take on clients on her own. She hired three more therapists over the years, and this year relocated the practice to Saratoga because it is central to where her clients live and is near the freeway.
“The area is beautiful, and there’s a need for what we do in the South Bay,” she said.
A big believer in continuing education, Johnson said she provides a budget for her therapists to receive continuing education. They also meet weekly to review cases.
“We have a really strong passion for what we do,” she said. “I originally got involved with CBT (cognitive behavior therapy) on my own because it helped me with my struggles back in the 1990s, and when I became a therapist I knew exactly what I wanted to do.”
The cost of each session varies by therapist, but ranges from $150 to $210. Most treatments require anywhere from 12 to 20 sessions over a period of three to six months. However, Johnson acknowledged that it really depends on the individual.
“Some people get results quickly, some have to come longer,” she said.
The Cognitive Behavior Therapy Center is at 12961 Village Drive, Suite C, Saratoga.
Anxiety disorders no joke
“Oh, that is just so OCD; I mean she is totally obsessed with her new phone.” “I swear I had a panic attack when I heard…”
How easily people make light of things about which they know very little, inadvertently but painfully mocking what causes others prolonged suffering. Yet to the millions of Americans who live with them, anxiety and panic disorders are no joke. Obsessive compulsive disorder, panic attacks, and phobias are types of anxiety and panic disorders which range from mildly disturbing to so disabling that leaving home becomes impossible.
May is Mental Health Awareness Month.
Obsessive-compulsive disorder (OCD) traps people in endless cycles of repetitive thoughts and behaviors. The approximate four million Americans with OCD are plagued by recurring and distressing thoughts, fears, or images (obsessions) which they cannot control. The resulting anxiety becomes an urgent need to perform certain rituals or routines (compulsions) in an almost subconscious attempt to get rid of the obsessive thoughts, but just temporarily. The cycle always repeats eventually and may progress, taking seconds or hours and interfering with normal activities. People with OCD may be aware of their obsessions and compulsions, but can’t stop them.
The symptoms of OCD vary, but commonly include exaggerated fears such as being dirty or contaminated by germs, causing harm to another, making even small mistakes, social embarrassment, or thinking “sinful” thoughts. Also fairly common is a need for order, symmetry, or exactness (peas on a plate or pencils lined up just so, to the point of being unable to concentrate or otherwise act without this), or excessive doubt and the need for constant reassurance.
Common compulsions include repetitive or constant bathing, hand-washing, rearranging items, and double-checking (e.g., stoves and locks), or needing to perform certain tasks a certain number of times (e.g. always knock three but not four times, or tap each doorway twice before entering), or perhaps refusing to shake hands or touch doorknobs. The compulsion may be body-related, such as specific coughing, throat-clearing, or making certain sounds (to oneself or aloud) and eating foods in a specific order. Also common is being stuck on certain words, phrases, or disturbing images – this may last all day and interfere with sleep.
While environmental factors such as abuse or trauma can be related to or trigger anxiety and panic disorders (or at least make them worse), biological factors have also been connected, perhaps more strongly in the case of OCD. Low serotonin is one example. Serotonin – a neurotransmitter which helps ferry messages from one neuron in the brain to another – imbalances may also be genetically passed on from parent to child, even if the same condition may not appear in both persons, or at least not as obviously.
Panic disorder (including panic attacks), while it is sometimes diagnosed along with OCD in the same person, is a distinct disorder. This is more than mere anxiety, nervousness, or elevated blood pressure in a tense situation. In fact, people who suffer from panic attacks also have them without any apparent outside cause. A person in the grip of a panic attack typically feels some combination of a sudden onset of nausea, dizziness, or sweating; difficulty breathing; a thumping in the chest; and an overall frightening feeling perhaps as severe as being near death. It’s very scary, very intense, and very sudden. They generally last 20 minutes or less, but in severe cases can last hours or days.
Yes, sometimes people with PTSD, such as veterans or other victims of violence, experience panic attacks. But many who suffer from them have not had such experiences. Because they are worried about experiencing an attack in social situations, people who have them commonly avoid crowds such as weddings or parties, fearful of being in a situation with too many witnesses of an embarrassing state, or feeling vulnerable. People with panic disorders often feel very isolated and alone.
This avoidance may simply be practical or related to agoraphobia (fear of open spaces or crowds) – which is chicken or egg is not always obvious. People who are phobic may also have panic attacks.
And what of phobias? They may or may not be rooted in a conditioning event, such as a fear of dogs beginning after a bite. The subject of the phobia, or fear, may, or may not, be of things average people avoid, such as rowdy crowds, spiders, snakes, or flying. In any case phobic fears are exaggerated and can be disabling, isolating people so they are afraid to leave home, enter a building, or be in the same environment as the subject of fear.
Phobias are far more than discomfort. They can make the 8 percent of Americans who are phobic visibly shake, faint, or feel in physical danger. It’s a mistake to tell a phobic or panicking person there is no reason to be afraid; implying their fear is irrational (which they likely already know) simply makes them feel more isolated and anxious. Help them breathe in and out slowly, leave with them to a quiet and safer-feeling place, stay with them until they feel calmer.
These conditions can not simply be willed away. People with severe anxiety and panic disorders may also experience chronic depression, aware of their conditions but feeling powerless to change them.
Anxiety and panic disorders are medical; they are not a sign of weakness. They are serious and involuntary, but they can be treated and improve. Treatments generally involve medication, such as anti-depressants which boost serotonin levels, and cognitive/behavioral therapies. For more information on these and other mental disorders, see NIMH.NIH.gov. For help, referrals, and connections to local support call the National Alliance for the Mentally Ill (NAMI) helpline (800) 950-NAMI.
Sholeh Patrick is a columnist for the Hagadone News Network. Contact her at sholeh@cdapress.com.
Scientists find genetic marker for obsessive-compulsive disorder, may lead to …
Researchers identified a genetic marker associated with obsessive-compulsive disorder, a mental disorder that affects millions of Americans. This could pave the way for development of a drug that could treat the condition.
(Photo : Wikimedia Commons)
Obsessive-compulsive disorder, an anxiety disorder estimated to affect about one in 100 adults or up to 3 million adults in the United States, is characterized by intrusive thoughts that cause worry, fear and a perceived need to do rituals and engage in certain thoughts. People with OCD may excessively wash their hands, do repetitive tasks and have aversion to certain numbers, behaviors that may cause distress and affect their way of life.
Current treatments for OCD include behavioral therapy and selective serotonin reuptake inhibitors (SSRI), but these do not work at all time and only address the symptoms of the disease. In what could potentially lead to the development of a drug treatment for OCD, researchers have identified a genetic marker that may be linked with the development of OCD.
In the study published in the journal Molecular Psychiatry on May 13, researchers scanned the genomes of 1,406 individuals with OCD and those of more than 1,000 parents whose children have the disorder to look for a certain genetic marker associated with OCD.
Study author Gerald Nestadt, from the Johns Hopkins University School of Medicine, and his colleagues identified a genetic marker found near the protein tyrosine phosphokinase (PTPRD) gene as it was more prevalent among participants with OCD than those in the control group. The PTPRD gene is notably associated with learning and memory, which are influenced by OCD. It is also linked with attention-deficit hyperactivity disorder (ADHD), a condition that shares some symptoms with OCD.
The researchers, however, said that although they have found a genetic marker, they still need to find the exact variant linked with OCD to determine the genetic cause of the disorder. Nestadt explained that a genetic marker is not often the cause of abnormality, albeit it tells that something near it may be the object of interest.
“The idea is that if we know what chemical or protein is affected in the condition,” Nestadt said, “then we can work out what problem is in the brain that causes the condition and the next step is to find a pharmaceutical that changes that or affects that so as to improve the condition.”
New Distinction of OCD Subtypes May Benefit Future Diagnosis, Treatment

A Michigan doctor and his colleagues say they are beginning to be able to identify distinct subtypes of childhood obsessive compulsive disorder which may benefit and improve the future diagnosis and treatment of OCD.
Dr. Rosenberg and colleagues at Wayne State University and the Detroit Medical Center’s Children’s Hospital of Michigan are beginning to define several different subtypes of OCD.
For example, Rosenberg and colleagues have found significantly different brain patterns in children with OCD who repetitively wash their hands than in children with OCD who repetitively check to make sure the door is locked.
“We see different things in the brain, and they respond differently to treatment,” Rosenberg told ABC News’ “20/20.”
Rosenberg said abnormalities in the brain chemical, glutamate, predict abnormalities in brain structure and chemistry and appear to differ based on the specific subtype of OCD. Abnormalities in specific glutamate genes appear to lead to brain glutamate abnormalities that can be measured with an MRI.
RELATED: Teen With OCD Overcomes Fear of Leaving His House to Attend Prom
In his team’s groundbreaking study looking at the MRIs of children who have OCD, Rosenberg said they are able to see the disorder in the children’s brains and that the brain chemical glutamate is critically involved in OCD.
“There’s too little glutamate in certain areas of the brain. There’s too much glutamate in other areas of the brain,” Rosenberg said.
According to Rosenberg, glutamate controls the brain’s light switch, and when the balance of glutamate is off in the brain, the light switch short circuits. Therefore, the part of the brain that gives most people the all clear when they’re worried never gives a child with OCD that same reassuring message.
RELATED: Living With OCD: The Lifelong Battle for Control Over the Disorder
“The key is that the light switch of the brain isn’t working properly and that just causes the whole system to go haywire, misfire,” Rosenberg said. “Instead of getting the signal that ‘Okay, I’m safe now,’ children with OCD get the signal that things are getting much more dangerous and unsafe.”
Rosenberg’s clinic and other clinics across the country are using glutamate targeted medicines clinically as part of the treatment of treatment resistant OCD. Further testing and clinical trials are being initiated and planned.
“This type of work is giving hope to a class of patients that there was no hope,” Rosenberg said.
Determining what causes OCD, Rosenberg said, is vital to better diagnose and treat the disorder because that knowledge heals and defeats ignorance and stigma.
Rosenberg cautions that not all patients with OCD will respond to glutamate modulating medicines, noting the importance of identifying and better characterizing specific brain subtypes of OCD.
RELATED: Resources for Families Seeking Treatment for Anxiety, OCD
For the past five years, ABC News’ “20/20” has followed the progress of children being treated for OCD, including Bridget, whose fear that her family was contaminated kept her from hugging her own mother. Another child, Rocco Decorso, struggled to leave the house because of the dangers he feared were waiting outside.
Rosenberg is convinced that Bridget, Rocco, and other children like them can conquer their OCD. Now that they can make the distinction between different subtypes of OCD based on where and how much glutamate they find in the brain of child with OCD, Rosenberg said they believe it will lead to new ways to both better diagnose and treat the disorder.
Watch “The Children Who Break Away” on ABC News’ “20/20” TONIGHT at 10 p.m. ET
Living With OCD: The Lifelong Battle for Control – WLS
Elizabeth McIngvale-Cegelski, Ph.D., LMSW, was diagnosed with obsessive compulsive disorder as a child. In an effort to help those living with OCD and other illnesses, McIngvale-Cegelski made it her life’s mission to ensure they receive treatment and to decrease the stigma that she said is associated with mental illness. Now 27, McIngvale-Cegelski received her Ph.D. in social work from University of Houston last week. She recently shared her daily battle with OCD with ABC News’ “20/20.”Watch her story and more on “The Children Who Break Away” on ABC News’ “20/20” on Friday, May 23, at 10 p.m. ET
Aren’t your teenage years supposed to be carefree and fun? Little did I know that would be the furthest from the truth for me.
By age 13 I was lost, scared and alone living with a crippling anxiety disorder what I soon would find out was obsessive compulsive disorder, also known as OCD.
I was taunted by intrusive thoughts that never seemed to end unless I ritualized — doing task over and over and over for hours at a time. Basic things like washing my hair had to be repeated until I thought it was done correctly. I would scrub my hands until the skin was raw. One round was never enough. The frustration was overwhelming. I would get so mad that I would punch holes in my bedroom wall. The disorder took over my life, my freedom and my happiness.
My family and I searched for help but couldn’t find it. In fact we were told my case was too severe to be treated. As you can imagine this only left me feeling more frustrated and hopeless.
However, help was available and I was able to receive the treatment that I needed in order to regain control over my life that had been stripped away by OCD.
Exposure with response prevention (ERP) is the treatment that forever changed my life, teaching me how to effectively fight my OCD. When engaging in ERP you complete exposures (such as touching a doorknob) and then engage in ritual prevention (no hand wash), working your way gradually from your least challenging exposures to your most challenging exposures until you have control over your OCD.
My battle wasn’t easy and isn’t over. I still battle my OCD on a daily basis but I learned the tools needed in order to successfully manage my illness and the life that I deserve to live. Treatment for OCD is available and it can get better.
Besides treatment I feel the second most important thing you can do for yourself is to connect with someone else living with OCD. Meeting someone else who understands what you are going through can help erase those feelings of loneliness that are often associated with a mental illness. It can help you know that you are not alone and there are others who have or are struggling as well. After treatment, I quickly decided that I would start telling my story in the hopes that it might help one other person living with OCD or any mental illness. I found this to be one of the greatest therapies for me. It helped me understand that I didn’t have to live in silence and hide my struggles. I decided to share my story with others and the world in an attempt to decrease the stigma associated with mental illness and OCD. This catapulted me into my current career, it helped me see first-hand that this is my passion and find a way to turn my battle into a way to help and impact others living with this illness and other illnesses. I have recently graduated with my Ph.D. in social work and will continue to make it my life’s mission to keep doing the work that I do until all with OCD can receive the treatment they deserve and until the stigma associated with mental illness no longer exists. Remember that you don’t have to suffer in silence, it can get better and both help and support are available.
For more information about OCD:
Visit the International OCD Foundation’s website here.Find an OCD support group here.
Visit Elizabeth’s nonprofit foundation here and her free self-help website for OCD here.
Found: Genetic Marker for Obsessive Compulsive Disorder
Researchers at Johns Hopkins University School of Medicine and colleagues have identified a genetic marker for obsessive compulsive disorder or OCD. If confirmed, the research could lead to development of drugs that could reduce the severity of this crippling, yet least understood mental disorder.
Obsessive-compulsive disorder is a type of anxiety disorder and affects around 2.2 million American adults. The mental illness can interfere with daily activities and cause severe distress. Media often shows OCD as some ‘quirky habit’ such as counting things or being careful about sequences or patterns. Cameron Diaz, for example, is rumored to use elbows to open doorknobs to avoid touching the knobs.
Share This Story
However, the disorder is a lot more complex. Obsession in the term OCD refers to frequent upsetting thoughts such as imagining harming or killing loved ones. Compulsions are a set of rituals or behaviors that the person performs to control panic attacks. Common examples of compulsive behaviors include unnecessary unlocking and locking doors or washing hands for a specific number of times.
“If this finding is confirmed, it could be useful,” said study leader Gerald Nestadt, M.D., a professor of psychiatry and behavioral sciences at the Johns Hopkins University School of Medicine, according to a news release. “We might ultimately be able to identify new drugs that could help people with this often disabling disorder, one for which current medications work only 60 to 70 percent of the time.”
The team conducted a type of research called genome-wide association study. . GWAS studies examine the link between genes and specific traits (mostly used to study human disease). In this study, researchers scanned the genome of 1,400 people with OCD and 1,000 close relatives of people with the condition. Researchers found that a gene called protein tyrosine phosphokinase (PTPRD) had links with OCD.
Research conducted on animals has shown that the gene is involved in learning and memory. Also, the PTPRD gene is linked to Attention Deficit Hyperactivity Disorder, another mental disorder that shares some of the symptoms of OCD, Nestadt said. Additionally, the gene along with another gene family, SLITRK has been implicated in OCD in animals.
“OCD research has lagged behind other psychiatric disorders in terms of genetics,” Nestadt said in a news release. “We hope this interesting finding brings us closer to making better sense of it-and helps us find ways to treat it.”
The study is published in the journal Molecular Psychiatry.
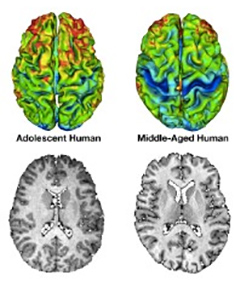
Obsessive-Compulsive Disorder and the Teen Brain
 When my son Dan was at a residential treatment program to battle his severe obsessive-compulsive disorder, my husband and I were encouraged by the staff there to let him make his own major life decisions, without any input from us.
When my son Dan was at a residential treatment program to battle his severe obsessive-compulsive disorder, my husband and I were encouraged by the staff there to let him make his own major life decisions, without any input from us.
This didn’t make sense to us and we consulted Dan’s therapist outside of the program, who said, “But he’s only 19. His frontal lobe development won’t even be complete until he’s 24. Of course he needs your guidance with these decisions.” Specifically, Dan had decided to leave college so he could stay “as long as possible” at the residential treatment program. Thankfully, we did intervene, and Dan left the program after a nine-week stay. He returned to college.
Before this discussion with my son’s therapist, I had never realized there is a biological reason why teens and young adults think and act the way they do, often exasperating their parents. The frontal lobes, the parts of the brain that typically ask: “Is this a good idea? What is the consequence of this action?” are not fully connected in teens and young adults.
My guess is anyone who has parented a teenager is now nodding his or her head in agreement. Now that I understand a little more about brain development in teens, I realize they actually have somewhat of an excuse for acting the way they do.
So what does this mean for teens and young adults with obsessive-compulsive disorder? Well, not only are these young people battling OCD, they are also dealing with their not-yet-completely developed brains. Both of these factors often involve a lack of good judgment as well as the inability to make smart decisions.
It’s a double whammy. And for parents and other loved ones of teens suffering from OCD, it can also be doubly challenging. In Dan’s case, we were fortunate he was never an antagonistic teen, but I still often found myself shaking my head in disbelief: “What was he thinking?” Was it his OCD or his age that caused him to think and act a certain way? Was it both? Or neither? Who knows?
Decision-making and impaired judgment are not the only deficits experienced by a “young” brain. I’ve previously written about the fact that teens experience more difficulty in overcoming fear than adults and children. This finding might help explain the surge in anxiety and stress-related disorders during adolescence, as there is actually a physiological reason why teenagers do not handle stress well. Not surprisingly, this can acutely affect their OCD, as well as their treatment success. Of course, if OCD is present and diagnosed in childhood, treatment early on can help ease the chaos of the teen years.
I think it’s important to keep in mind that we should not automatically “blame” OCD for all the frustrating behavior in teens and young adults with the disorder. I actually find that comforting in a way; some of the baffling behavior our teens and young adults exhibit should diminish with age. And the rest? Well, hopefully, exposure and response prevention therapy, the frontline treatment for OCD, will do the trick.
Last reviewed: By John M. Grohol, Psy.D. on 19 May 2014
Published on PsychCentral.com. All rights reserved.

Short OCD Quiz May Spot Anxiety and Depression
 Emerging research suggests a shortened version of a questionnaire used by psychologists to assess risk factors for obsessive-compulsive disorder also may help determine the risk of depression and anxiety.
Emerging research suggests a shortened version of a questionnaire used by psychologists to assess risk factors for obsessive-compulsive disorder also may help determine the risk of depression and anxiety.
The condensed tool may be useful for assessing the risk of mental health issues stemming from certain beliefs — such as seeing threats as greater than they are and feeling that things are not right unless they are perfect.
Such dysfunctional beliefs are central to obsessive-compulsive disorder (OCD), said researcher Thomas Fergus, Ph.D., assistant professor of psychology and neuroscience in Baylor’s College of Arts and Sciences.
The initial Obsessive Beliefs Questionnaire, developed in 2001 and consisting of 87 items, has been revised and shortened three times, most recently in 2011, with the goal of making it more practical for use.
“It now has only 20 items, but the concepts have not been changed,” Fergus said.
Those with obsessive-compulsive disorder tend to overestimate threats, have an inflated sense of responsibility, be perfectionists and fear intrusive thoughts because they feel out of control.
Symptoms of OCD include such behavior as excessive washing or repeated checking.
“At one time, the questionnaire was used because it was thought that responsibility or overestimation of threat might be specific to OCD,” Fergus said.
“But the short of it now is that certain beliefs appear to be relevant for more than OCD, so this might help us better understand depression and anxiety and have a broader application.”
The new research included two studies. In the first, participants were 48 patients who came to an outpatient clinic for stress and anxiety disorders, while in the second, 507 non-clinical adults were recruited through the Internet.
In the first study, participants were given both the original, longer version of the questionnaire and the 20-item version, with similar results found using each version.
In the second study, participants were given the shorter Obsessive Beliefs Questionnaire; a questionnaire used to assess obsessive-compulsive symptoms; a questionnaire used to determine depression symptoms; and another to assess general anxiety.
That study revealed similarities in beliefs related to OCD, depression and anxiety.
“Given the brevity of the revised Obsessive Beliefs Questionnaire — and its potential for patients — it could become a useful tool for research as well as treatment of patients and intervention for those who are predisposed toward a number of mental health disorders,” Fergus said.
The study was published in the Journal of Psychopathology and Behavioral Assessment.
Source: Baylor University
Patient completing questionnaire photo by shutterstock.
<!–
Advocacy and Policy, Anxiety, Brain and Behavior, Depression, General, Health-related, LifeHelper, Memory and Perception, Mental Health and Wellness, OCD, Personality, Psychology, Research, Social Phobia, Social Psychology, Stress
–>
Obsessive-compulsive disorder questionnaire may give clues to other mental …
A shortened version of a questionnaire used by psychologists to assess risk factors for obsessive-compulsive disorder also may help determine the risk of depression and anxiety, according to a Baylor University study.
The revision may be a good fit for assessing the risk of mental health issues stemming from certain beliefs—such as seeing threats as greater than they are and feeling that things are not right unless they are perfect. Such dysfunctional beliefs are central to obsessive-compulsive disorder (OCD), said researcher Thomas Fergus, Ph.D., assistant professor of psychology and neuroscience in Baylor’s College of Arts and Sciences.
The study was published in the Journal of Psychopathology and Behavioral Assessment.
The initial Obsessive Beliefs Questionnaire, developed in 2001 and consisting of 87 items, has been revised and shortened three times, most recently in 2011, with the aim of making it more practical for use. It now has only 20 items, but the concepts have not been changed, Fergus said.
Those with obsessive-compulsive disorder tend to overestimate threats, have an inflated sense of responsibility, be perfectionists and fear intrusive thoughts because they feel out of control. OCS symptoms include such behavior as excessive washing or repeated checking.
“At one time, the questionnaire was used because it was thought that responsibility or overestimation of threat might be specific to OCD,” Fergus said. “But the short of it now is that certain beliefs appear to be relevant for more than OCD, so this might help us better understand depression and anxiety and have a broader application.”
The research included two studies. In the first, participants were 48 patients who came to an outpatient clinic for stress and anxiety disorders, while in the second, 507 non-clinical adults were recruited through the Internet.
In the first study, participants were given both the original, longer version of the questionnaire and the 20-item version, with similar results found using each version.
In the second study, participants were given the shorter Obsessive Beliefs Questionnaire; a questionnaire used to assess obsessive-compulsive symptoms; a questionnaire used to determine depression symptoms; and another to assess general anxiety. That study revealed similarities in beliefs related to OCD, depression and anxiety.
Given the brevity of the revised Obsessive Beliefs Questionnaire—and its potential for patients—it could become a useful tool for research as well as treatment of patients and intervention for those who are predisposed toward a number of mental health disorders, Fergus said.
![]()
Explore further:
Researchers identify genetic marker linked to obsessive-compulsive disorder
![]()
![]()
![]()
![]()